How to Identify Visceral Referred Pain on the Thoracic Wall
When a patient complains of chest discomfort, the source is not always the heart or lungs. Visceral organs often “refer” pain to the thoracic skin, creating a misleading picture. Understanding the map of referred pain lets clinicians separate cardiac red flags from gastrointestinal clues, speeding up diagnosis and avoiding unnecessary tests.
Why does pain travel from internal organs to the chest wall?
Visceral structures share spinal segments with the intercostal nerves that supply the skin. When an organ such as the stomach, gallbladder, or pancreas becomes irritated, the spinal cord receives the signal on the same “address” as the skin over the corresponding rib space. The brain then interprets the sensation as coming from the skin—a phenomenon called visceral referred pain. Recognising this neural overlap helps you trace the discomfort back to its true origin.
Which thoracic zones correspond to specific organs?
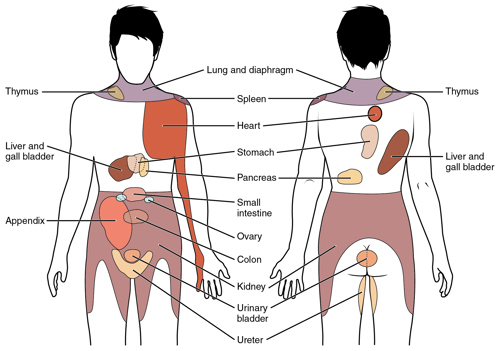
The illustration above divides the thorax into zones linked to common visceral sources. For example, pain at the left lower ribs (T7‑T9) often signals a gastric ulcer, while right‑side discomfort near the 9th‑11th ribs may indicate gallbladder inflammation. Lower thoracic segments (T10‑T12) correspond to the pancreas, duodenum, and even the colon. By matching the patient’s pain location with this map, you can narrow the differential diagnosis before ordering imaging.
How can a step‑by‑step assessment differentiate cardiac from visceral causes?
- History first. Ask the patient to describe the pain’s onset, radiation, and aggravating factors. Cardiac pain usually worsens with exertion and is pressure‑like, whereas visceral pain may be dull, crampy, or triggered by meals.
- Physical exam. Palpate the corresponding intercostal spaces. Tenderness that reproduces the pain suggests a somatic component, while a soft, non‑tender area leans toward visceral origin.
- Vital signs. Elevated heart rate, blood pressure spikes, or abnormal ECG findings point to cardiac involvement.
- Diagnostic tests. If the pain pattern matches a visceral zone and cardiac work‑up is negative, consider labs (e.g., amylase for pancreatic pain) or abdominal ultrasound.
What practical notes should beginners keep in mind when using the pain map?
- Don’t rely on a single spot. Patients often feel pain in more than one intercostal space; note the most intense area.
- Combine with the “road‑sign” test. Pressing on the intercostal space may reproduce visceral pain because the same spinal segment is activated.
- Remember age‑related variation. Elderly patients may have atypical presentations, so a broader assessment is essential.
- Document the exact rib level. Using “T‑number” terminology (e.g., T8) creates a common language for referrals.
When should you still suspect cardiac disease despite a visceral pattern?
Even when the pain aligns with the referred‑pain map, certain red flags demand immediate cardiac evaluation. Sudden onset, radiating to the left arm or jaw, associated diaphoresis, or a history of coronary artery disease cannot be dismissed. In such cases, treat the presentation as cardiac until proven otherwise, then revisit the visceral possibilities once life‑threatening causes are excluded.